How To Treat Bipolar Depression In Pregnancy
Women with particularly brittle bipolar disorder or with histories of response to lithium may in consultation with their doctors consider use of lithium during pregnancy given the almost 50-year history of data accumulation on its reproductive safety compared with some of the other mood stabilizers for which there is either confirmed teratogenicity sodium valproate or still incomplete data. Bipolar Disorder and Postpartum Depression.
:max_bytes(150000):strip_icc()/bpd-vs-bipolar-5096132_FinaL-e946be6d6df04527a2a043e6e974abd0.jpg) Bpd Vs Bipolar Symptoms And Treatment
Bpd Vs Bipolar Symptoms And Treatment
Lithium and bipolar pregnancy.

How to treat bipolar depression in pregnancy. New mothers with bipolar disorder are more likely to have PPD and bipolar disorder may be more likely to. The treatment of bipolar disorder in pregnant women involves significant challenges. Some medications used to treat Bipolar disorder are.
Managing bipolar disorder often means taking. Carbamazepine is usually only prescribed on the advice of an expert in bipolar disorder. The treatment of pregnant women with bipolar disorder is challenging.
Studies show that exposure to only one mood stabilizer during pregnancy is less harmful to the developing fetus than exposure to multiple medications. Those who have had a previous severe postpartum illness. Therefore about half of women with bipolar disorder stay well after having a baby and about half may have an episode of illness.
Management requires sustained collaboration between the patients family physician and her psychiatrist. Valproate is not usually prescribed for women of childbearing age because theres a risk of physical defects. Bipolar disorder comes with its own unique challenges that include mood swings as a result of hormonal fluctuations during pregnancy shared Dr.
There is very little risk to the fetus when Lithium levels are monitored closely. While medications help to improve mood stability during pregnancy these medications could also lead to potential birth defects and complications. Maintenance pharmacotherapy for women with bipolar disorder during pregnancy is so important not only to decrease the risk of relapse following discontinuation of mood stabilizers but because recurrence of illness during pregnancy for these patients is a very strong predictor of risk for postpartum depression.
Your doctor and your obstetrician may decide to stop or lower your medications during your pregnancy during which time you will have to rely on other forms of treatment for managing your bipolar disorder such as psychotherapy and self-care. Be sure to talk with both your obstetrician and psychiatrist about the risks and benefits of bipolar medications and forms of birth. Relapse rates are high in the setting of medication discontinuation.
Several of the medications used as mood stabilizers specifically lithium and valproic acid carry some teratogenic risk. Lithium is a common medication used to treat Bipolar disorder. The issues for pregnant women using lithium to treat bipolar are mainly about timing.
Two groups of women with bipolar disorder are at even higher risk. Postnatal depression follows a further 25 of births. Not had previous psychiatric illness.
Mothers who are on other Bipolar medications. Ents in decisions regarding pregnancy termination and perinatal interventions after delivery. The course of bipolar disorder during pregnancy is variable.
Based on everything we know about bipolar and pregnancy the plan should be detailed and specific so there is a definite strategy planned for each week for example resuming lithium in week 9 if there are signs of relapse. To reduce risk to the fetus its optimal to prevent bipolar relapse and expose the unborn child to as few bipolar medications as possible. On the other hand the teratogenicity associated with lithium may have been overestimated in the past.
You may also consider. Continuing with bipolar treatment during pregnancy may lower the risk of relapse after giving birth. Perhaps you have bipolar disorder and do not want a pregnancy.
As a result some people choose not to take mood-stabilizing medications while. Limiting the number of manic and depressive episodes you have will help you function at your best each day. Learn more about Bipolar Disorder Medications.
Some of these anticonvul-sant agents represent more potent teratogenic risks than lithium. Electroconvulsive therapy ECT regular exercise to naturally boost serotonin the feel-good hormone talk therapy cognitive behavioral therapy support groups omega-3 fatty acids like flax seed in addition to eating a couple of servings a. Anticonvulsants A number of anticonvulsants most notably sodium val-proate and carbamazepine have been used in the acute treatment of bipolar disorder.
Some mood stabilizers eg sodium valproate and carbamazepine are human teratogens.
 Pin On Mental Health
Pin On Mental Health
 Integrative Treatment Of Bipolar Disorder A Review Of The Evidence And Recommendations
Integrative Treatment Of Bipolar Disorder A Review Of The Evidence And Recommendations
 Mardziatun Nisa On Instagram It Always Exhausted Its Like Never Ending Charging Of Battery And Still The Battery Is Low Wakeu Low Battery Exhausted Wake Up
Mardziatun Nisa On Instagram It Always Exhausted Its Like Never Ending Charging Of Battery And Still The Battery Is Low Wakeu Low Battery Exhausted Wake Up
 Pin On Grace
Pin On Grace
 Pregnancy Outcomes In Women With Bipolar Disorder Mgh Cwmh
Pregnancy Outcomes In Women With Bipolar Disorder Mgh Cwmh
 Pin On Self Care Recovery
Pin On Self Care Recovery
 Pin On Bipolar
Pin On Bipolar
 Pin On All About Pregnancy Birthing Women Childrens Parenting
Pin On All About Pregnancy Birthing Women Childrens Parenting
 Gaia Research Kelp Seaweed Kelp Gaia Port Elizabeth
Gaia Research Kelp Seaweed Kelp Gaia Port Elizabeth
Worse Pregnancy Outcomes In Women With Bipolar Disorder
 Pin On Natural Renedies
Pin On Natural Renedies
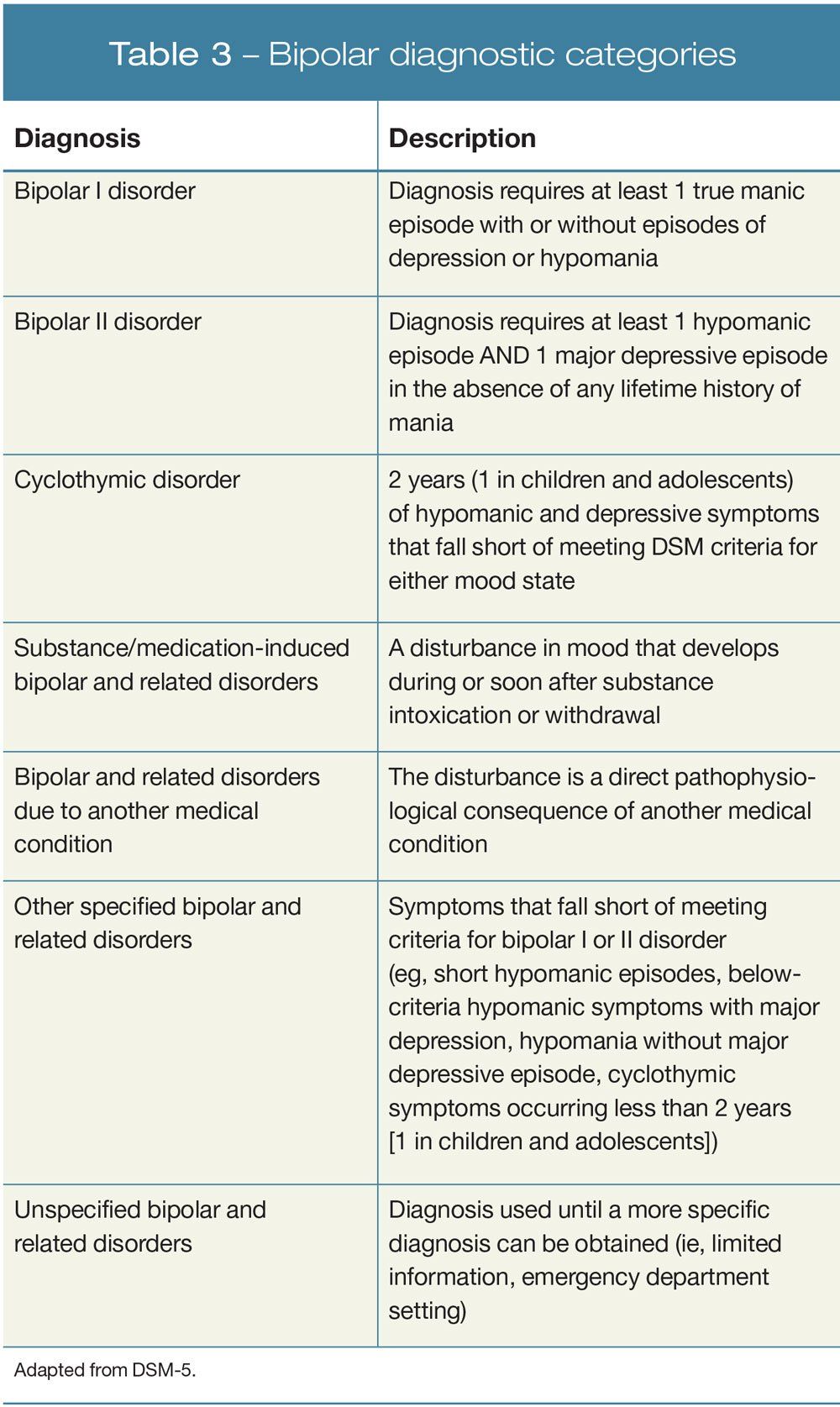 An Update On The Diagnosis And Treatment Of Bipolar Disorder Part 1 Mania
An Update On The Diagnosis And Treatment Of Bipolar Disorder Part 1 Mania
 Understanding Schizophrenia Schizophrenia Psychology Disorders Schizoaffective Disorder
Understanding Schizophrenia Schizophrenia Psychology Disorders Schizoaffective Disorder
 Bipolar Pregnancy Risks What To Expect And More
Bipolar Pregnancy Risks What To Expect And More
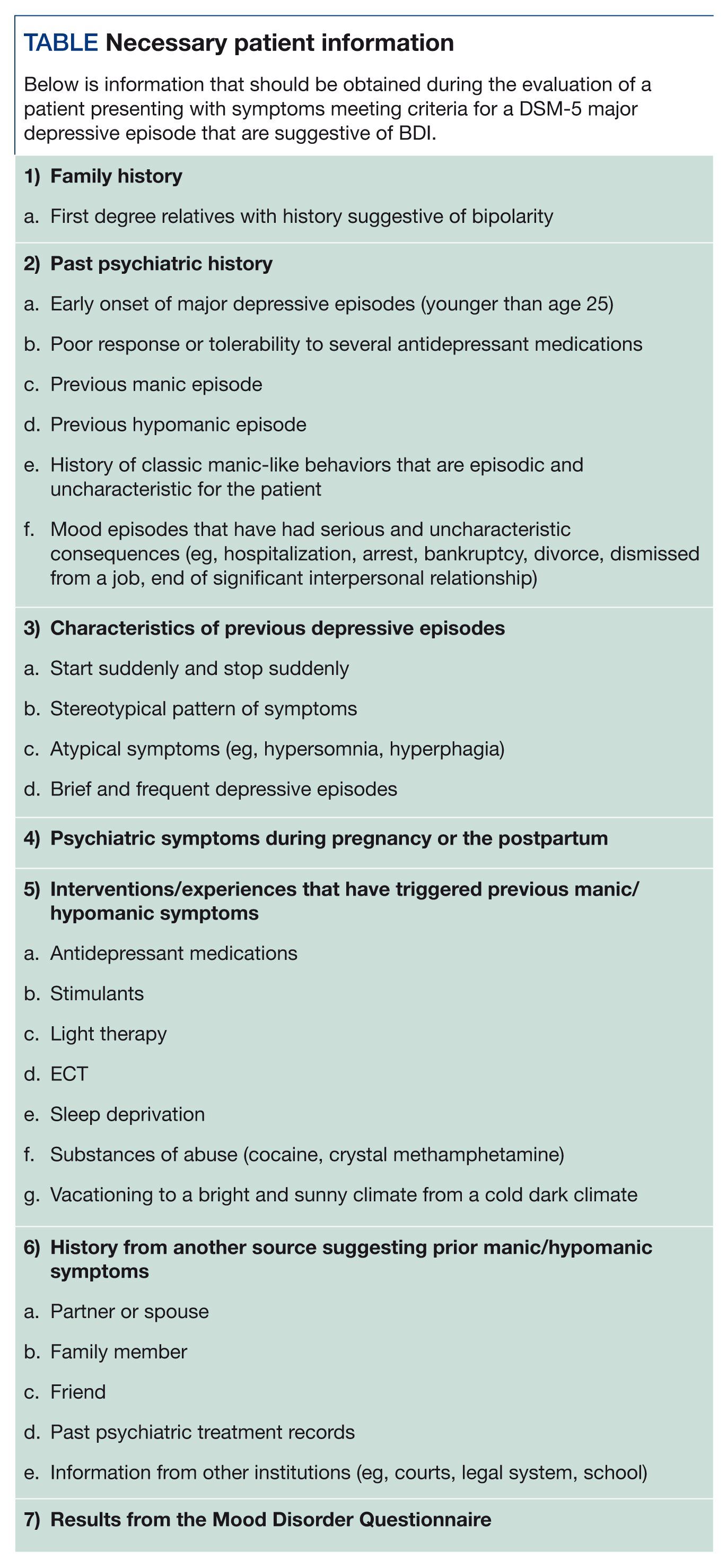 Major Depressive Episode Is It Bipolar I Or Unipolar Depression
Major Depressive Episode Is It Bipolar I Or Unipolar Depression

 Minocycline And Celecoxib As Adjunctive Treatments For Bipolar Depression A Multicentre Factorial Design Randomised Controlled Trial The Lancet Psychiatry
Minocycline And Celecoxib As Adjunctive Treatments For Bipolar Depression A Multicentre Factorial Design Randomised Controlled Trial The Lancet Psychiatry
 Pin On Ppd Pmad News
Pin On Ppd Pmad News
 Cope Bipolar Disorder In Pregnancy
Cope Bipolar Disorder In Pregnancy
:max_bytes(150000):strip_icc()/bpd-vs-bipolar-5096132_FinaL-e946be6d6df04527a2a043e6e974abd0.jpg&description=How To Treat Bipolar Depression In Pregnancy){kind=link}
Post a Comment for "How To Treat Bipolar Depression In Pregnancy"